


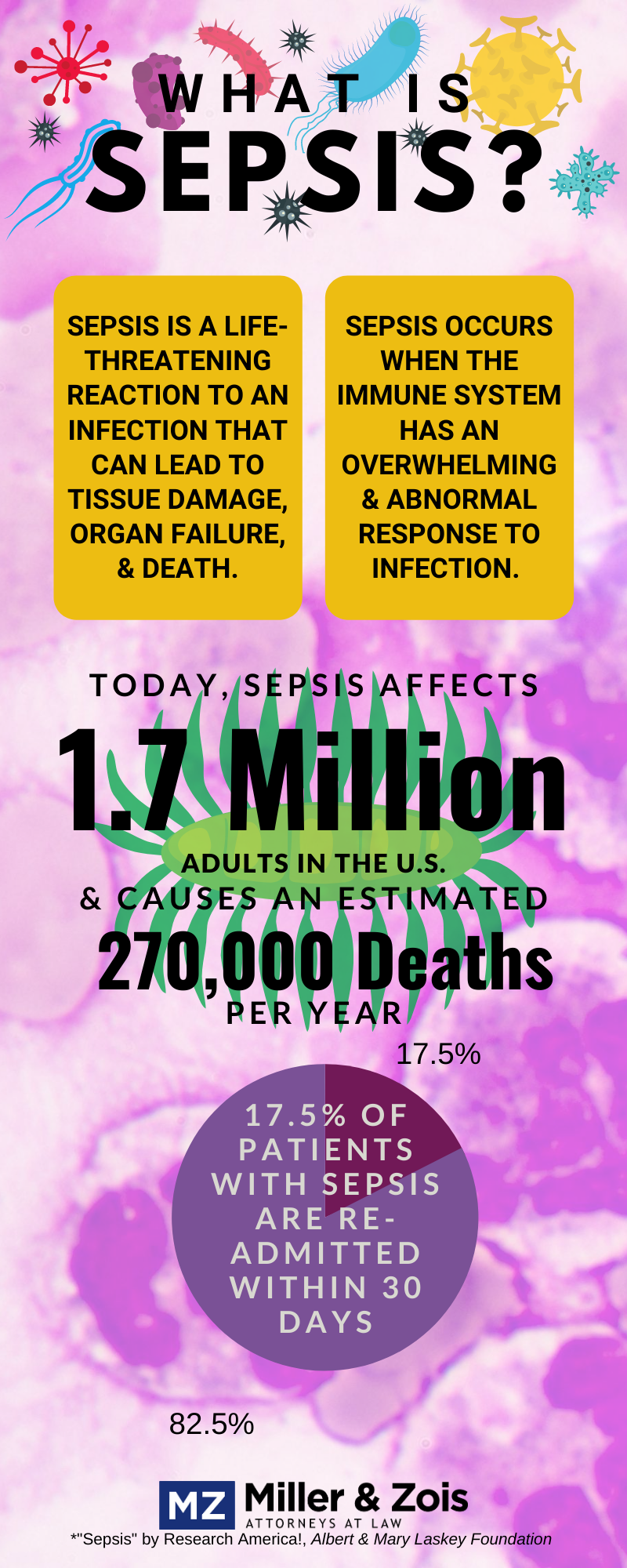
Sepsis is a silent killer that should be diagnosed and treated with the same urgency as a heart attack. But it is not treated with urgency, making it is the one reason why so many medical malpractice lawsuits in Maryland involve either missed sepsis diagnosis or a failure to adequately treat this infection. Sepsis is a catastrophic health problem responsible for over 250,000 deaths per year in this country. There are over 20,000 cases of sepsis in Maryland hospitals every year. Do you think Donald Trump’s wall is too expensive? We spend more $20 billion dollars on the diagnosis and treatment of sepsis. It is the most expensive condition treated in hospitals and a lot of that cost is care rendered after a doctor makes a mistake. Sepsis is an infection of the bloodstream from some other source. Severe sepsis can cause organ failure that can kill you. These are the symptoms of sepsis that should give put doctors and hospitals on alert:
Maryland involve either missed sepsis diagnosis or a failure to adequately treat this infection. Sepsis is a catastrophic health problem responsible for over 250,000 deaths per year in this country. There are over 20,000 cases of sepsis in Maryland hospitals every year. Do you think Donald Trump’s wall is too expensive? We spend more $20 billion dollars on the diagnosis and treatment of sepsis. It is the most expensive condition treated in hospitals and a lot of that cost is care rendered after a doctor makes a mistake. Sepsis is an infection of the bloodstream from some other source. Severe sepsis can cause organ failure that can kill you. These are the symptoms of sepsis that should give put doctors and hospitals on alert:
- temperature greater than 100.4F or less than 96.8F
- white blood cell count greater than 12,000 or less than 4,000
- heart rate greater than 90
- decreased blood pressure
- respiratory rate greater than 20
- altered mental status
- low oxygen saturation
- Skin is cool, blue or mottled (because blood flow is reduced)
- failure of multiple organs
Many Malpractice Cases Begin with Ignored Symptoms
You can stop here for the birthplace of many Maryland wrongful death malpractice lawsuits. Often, failing to investigate the sepsis appropriately by, for example, getting an infectious disease consultation after these symptoms arise, can be a breach of the standard of care. But, really, it should not take an infectious disease doctor to know that any serious infection needs to be treated with antibiotics urgently and you have to make sure the patient does not have an infection. Maryland EMS’s have a protocol for sepsis. If there are 20,000 cases a year in Maryland, everyone who is seeing patients in a hospital or primary care setting has to be jumping on the symptoms to rule out sepsis. When two or more of these are met, it is time to act. The good news is doctors have a ton of weapons at their disposal that can help the patient. Antibiotics, blood cultures, and fluid resuscitation are just some of the many tools doctors can have to diagnose and treat. Antibiotics are a big deal. The correlation between the prompt administration of intravenous antibiotics and survival is very strong.
- Example of a sepsis misdiagnosis lawsuit against Kaiser in Montgomery County
- Another sepsis misdiagnosis case, this one against Holy Cross
- Sample verdicts and settlements in sepsis cases
Septic Shock
When we get to septic shock, the horse is getting out of the barn. Septic shock occurs when sepsis is not treated and the body cannot cope with the infection. The theory is that sepsis represents an over-exuberant inflammatory response in response to invading bacteria or other pathogens in which various mediators released by white blood cells and tissues cause excessive activation of host defense mechanisms. This results injury to the patient. If a patient has septic shock, antibiotics will not get the job done. The source of ongoing infection must be identified and removed before inflammatory mediated damage can be reversed.
How Defense Lawyer Fight These Cases
A lot of sepsis cases are “what or earth were these doctors thinking?” cases. So what do defense lawyers do? Well, many patients with sepsis have a complex medical history. So the go-to leitmotif you hear is that the patient was going to die no matter what. There seem to be some — perhaps not so coincidentally well paid by defense lawyers– infectious disease and critical doctors who think that just about anyone who does die would have died anyway. There is no question that there are cases where this defense is valid. Not all 250,000 sepsis deaths every year are from malpractice. But far too many of these cases are medical negligence claims. The good news for plaintiffs is that if the doctor’s defense is “even if I hadn’t screwed up this patient would have died anyway” their patented “I am a doctor and therefore infallible” defense is already laying on the courtroom floor. If the patient would not have died except for the misdiagnosis, you will be able to marshal powerful evidence to prove the patient would have lived. How do doctors try to get around missing the classic symptoms of sepsis? One common path is to say that the symptoms of sepsis are the same as many other serious ailments so they had reason to suspect something other than sepsis. This argument fails to understand that doctors can walk and chew gum at the same time. A differential diagnosis is to keep looking until you rule out possibilities. If you have a disease that kills 250,000 people every year, you want to keep that on your list of possibilities. You think the patient has pancreatitis? Fine. But keep testing to rule out sepsis. Defense lawyers also know that juries want to blame someone when something awful happens that should not have happened. In those cases, the tried and true defense is blaming the patient. They will say the patient failed to disclose a possible source of infection (often because the wrong questions were asked) or that the patient’s own poor health choices caused the infection. Usually, if the defense is digging down this deep, you are in a good position. These cases often either settle out-of-court or the jury sees it for just what it is.
Sepsis Misdiagnosis Verdicts and Settlements
YEAR / STATE
CASE / INJURY SUMMARY
RESULT
2019 – Florida
A 44-year-old woman’s surviving relatives alleged the medical staff’s failure to timely diagnose her MRSA-infected pneumonia caused her death from sepsis. The woman, who suffered from asthma, was admitted to the hospital for respiratory failure, an asthma attack, and hypertension. After being hospitalized for a week, her condition appeared to improve. However, she eventually experienced chest pain and shortness of breath. The staff then made a rapid response code call. The house physician responded to the call, ordered multiple tests, prescribed several medications, and diagnosed the woman with a myocardial infarction. However, the woman was later revealed to have suffered a severe lung infection instead. The following day, the staff made a second rapid response code call. The woman underwent a chest X-ray, which revealed an infected pleural effusion, a sign of pneumonia. The staff then administered Vancomycin to treat it. Despite undergoing treatments, the woman suffered a cardiac arrest from septic shock and died in the early morning. Her surviving relatives alleged that the hospital staff failed to timely diagnose the woman with MRSA-infected pneumonia. They claimed that the staff’s failure to administer blood tests before the first rapid response call caused the infection to progress. They also argued that she would have survived had the hospital staff administered antibiotics earlier on in her treatment. The jury awarded the family a $15,000,000 verdict.
$15,000,000 – Verdict
2020 – South Carolina
A 67-year-old man died from sepsis complications about ten days after he underwent a colonoscopy. A week after undergoing the procedure, he presented to the same physician with complaints of rectal bleeding and spasms, stomach cramps, and darkened urine. The physician referred him to the man’s primary care physician for an evaluation. Three days later, the man underwent an exploratory laparotomy that showed a colon perforation. He then underwent a colostomy that involved closing the perforation. After the procedure, the man developed kidney failure, liver failure, anemia from blood loss, and metabolic acidosis. This caused him to suffer peritonitis with sepsis, leading to multi-organ failure that resulted in his death. The case settled for $750,000.
$750,000 – Settlement
2020 – Pennsylvania
A 79-year-old woman, with a medical history of diverticulitis, alleged that the delayed diagnoses of her sepsis and peritonitis caused her to undergo multiple major surgeries. She presented to her primary care physician with abdominal pain complaints. The physician ordered a KUB diagnostic test, an EKG test, and a chest X-ray. The results revealed no medical issues. The woman’s abdominal pain eventually worsened, prompting her to visit the emergency room. She was diagnosed with sepsis, multiple digestive tract ruptures, intestinal perforation and necrosis, uterine perforation and necrosis, and peritonitis. As a result, she underwent multiple surgical procedures including a colostomy and a total hysterectomy. The woman sued her physician, his employer, and her treating hospital. She alleged that her physician failed to order an abdominal CT scan, despite knowing her diverticulitis history, which would have allowed for the timely treatment of her condition. The woman also alleged that the hospital staff’s mislabeling of her condition as gynecological caused delays in her care. She claimed that these delays caused a bust abscess that allowed infected fluid to leak into her abdominal and pelvic cavities, leading to permanent injuries. A jury awarded the woman a $700,000 verdict.
$700,000 – Verdict
2019 – South Carolina
A 7-month-old girl’s mother alleged that the physician’s failure to diagnose her intussusception and sepsis led to her death. The girl was initially brought to the emergency room for a bloody stool and vomiting. She received a viral gastroenteritis and nausea diagnosis and was discharged. Two days later, the girl vomited in the early morning. Her mother tried to bring her to her pediatrician, but she became unresponsive in the car. She died shortly after. An autopsy revealed that sepsis, secondary to intussusception caused her death. The mother alleged that the physician failed to order appropriate testing to properly diagnose her condition. The mother also alleged that the physician discharged her too early. This case settled for $1,000,000.
$1,000,000 – Settlement
2019 – Pennsylvania
An 85-year-old nursing home resident’s surviving family alleged that the delayed diagnosis of her urinary tract infection led to her death from sepsis. They sued the nursing home, alleging that they left the woman more infection-prone by failing to properly nourish and hydrate her. The surviving relatives also alleged that she developed a urinary tract infection that was left undiagnosed and untreated. They claimed that this led to sepsis, which caused her death. The facility denied negligence, alleging that her comorbidities led to her death.
$105,000 – Settlement
2019 – Florida
A 44-year-old woman’s surviving relatives alleged the medical staff’s failure to timely diagnose her MRSA-infected pneumonia caused her death from sepsis. The woman, who suffered from asthma, was admitted to the hospital for respiratory failure, an asthma attack, and hypertension. After being hospitalized for a week, her condition appeared to improve. However, she eventually experienced chest pain and shortness of breath. The staff then made a rapid response code call. The house physician responded to the call, ordered multiple tests, prescribed several medications, and diagnosed the woman with a myocardial infarction. However, the woman was later revealed to have suffered a severe lung infection instead. The following day, the staff made a second rapid response code call. The woman underwent a chest X-ray, which revealed an infected pleural effusion, a sign of pneumonia. The staff then administered Vancomycin to treat it. Despite undergoing treatments, the woman suffered a cardiac arrest from septic shock and died in the early morning. Her surviving relatives alleged that the hospital staff failed to timely diagnose the woman with MRSA-infected pneumonia. They claimed that the staff’s failure to administer blood tests before the first rapid response call caused the infection to progress. They also argued that she would have survived had the hospital staff administered antibiotics earlier on in her treatment. The jury awarded the family a $15,000,000 verdict.
$15,000,000 – Verdict