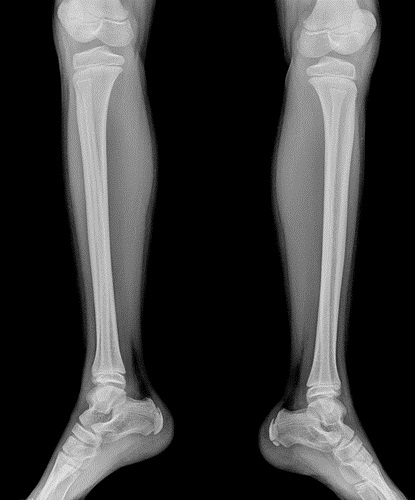
Jury Verdict Research published data on verdicts in severe leg injury cases over the 10 years prior to October 2010. By severe, I mean severe: crush injuries and amputations. For injuries to one or both legs, and leg injuries resulting in varying degrees of leg amputations, the statistics are:
Jury Verdict Research published data on verdicts in severe leg injury cases over the 10 years prior to October 2010. By severe, I mean severe: crush injuries and amputations. For injuries to one or both legs, and leg injuries resulting in varying degrees of leg amputations, the statistics are:
| INJURY |
AVERAGE |
MEDIAN |
| One or Both Legs |
$4,000,000 |
$2,400,000 |
The average verdict in these cases is approximately $4,000,000 and the median verdict is $2,400,000 for injuries to one or both legs, and leg injuries resulting in varying degrees of leg amputations.
The leg amputation categories include both traumatic and surgical amputations. The relatively insignificant difference surprised me between above the knee and below the knee amputations:
| INJURY |
AVERAGE |
MEDIAN |
| Above the knee |
$3,958,003 |
$2,588,649 |
| Below the knee |
$4,930,186 |
$3,727,500 |
| Bilateral Amputation |
$13,392,589 |
$5,012,500 |
As you can see, the median for bilateral amputations is a statistically insignificant difference from a single above the knee amputation.
This is interesting data and useful to use in negotiating your case. But asking the numbers to make sense is asking too much.
Settlements & Verdicts – Serious Leg Injuries
Below are summaries of cases resulting in verdicts or settlements where the primary injury was a serious leg injury,
Smith v. Elseroad (Baltimore City 2023) $425,000: The plaintiff was standing between two parked cars when the defendant motorist smashed his vehicle into the rear of one of the cars, pushing it forward into the plaintiff and crushing the plaintiff between the parked cars. The plaintiff suffered a bilateral leg crush injury resulting in permanent injuries, a right fibular head fracture, a permanent concave deformity on his calf, and permanent scarring on his lower body.
Hupp v. United States (D. Md. 2021) $729,000: Plaintiff suffered multiple fractures to his left ankle, requiring fusion and resulting in loss of motion and pain, as well as aggravation of preexisting condition, when the motorcycle he was operating was struck by a USPS mail truck that backed up from a parked position without warning, causing his left leg to be pinned under the motorcycle.
Johnson v. Bautista (Baltimore County 2021) $2,458,000: plaintiff suffered crush injuries to his right leg, including fractures to his right femur and tibia and nerve damage requiring surgery followed by physical therapy, and resulting in the permanent loss of feeling in his right foot and a combined right leg/lower extremity impairment rating of 46 percent. Jury awarded $208,000 in economic damages and $2.2 million for pain and suffering.
Thomas v. MTA (Baltimore City 2019) $1,200,000: plaintiff, a water taxi deckhand, suffered multiple fractures to her left leg and an open fracture of her left ankle, both of which required extensive surgeries, including placement of rods and screws and skin grafting, and resulted in extensive scarring on her leg. Case settled for $1.2 million.
Turner v. Brown (Baltimore City 2018) $390,394: plaintiff suffered a left leg hairline fracture, a left knee meniscus tear that required surgery when he was struck by a commercial vehicle driven by the defendant.
Patton v. Ruiz (P.G. County 2017) $1,584,296: plaintiff suffered right leg compound fractures, including a right knee fracture, resulting in persistent leg and knee pain and weakness and permanent radicular symptoms related to his leg and knee, when defendant allegedly made a left turn at an intersection on a steady red light and struck the plaintiff’s vehicle as it was proceeding through the intersection on a green light.
Koger v. Mabato (Baltimore City 2017) $1,203,013: Plaintiff was hit by a mobility bus in an intersection and suffered a fractured right distal femur, which required open reduction and internal fixation surgery and resulted in permanent impairment, as well as a fractured scapula, resulting in difficulty walking, standing, sitting and using stairs, continuing pain and permanent impairment of his right knee/leg.